
Services
Reflux Surgery (Fundoplication)
Reflux Surgery (Fundoplication)
Reflux surgery, also known as fundoplication, is a surgical procedure used to treat gastroesophageal reflux disease (GERD) and related conditions. GERD occurs when stomach acid frequently flows back into the esophagus, causing symptoms such as heartburn, regurgitation, chest pain, and difficulty swallowing. When lifestyle changes and medications fail to provide relief, surgery may be recommended.
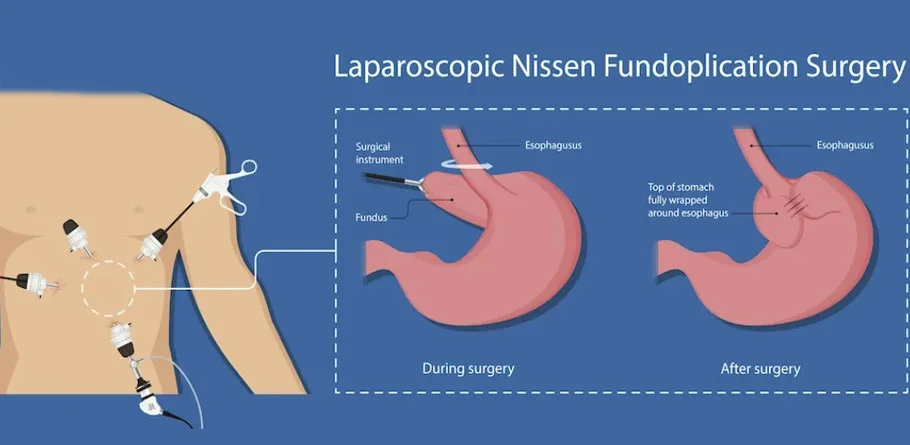
Fundoplication involves wrapping the upper part of the stomach (the fundus) around the lower esophagus to strengthen the lower esophageal sphincter (LES), the muscle that acts as a valve between the esophagus and the stomach. This wrapping helps prevent stomach acid from refluxing into the esophagus.
There are several types of fundoplication procedures, including:
- Laparoscopic Nissen Fundoplication: This is the most common type of fundoplication. It is performed using minimally invasive techniques, where several small incisions are made in the abdomen, and a laparoscope (a thin, flexible tube with a camera) and surgical instruments are inserted to perform the procedure.
- Laparoscopic Toupet Fundoplication: This is similar to the Nissen fundoplication but involves a partial wrap of the stomach around the esophagus.
- Laparoscopic Dor Fundoplication: This procedure involves wrapping the stomach around the esophagus in a different manner compared to the Nissen and Toupet procedures.
Bariatric Surgery
Bariatric Surgery
Bariatric surgery, also known as weight loss surgery, is a medical procedure performed on individuals who are severely overweight or obese, typically when other weight loss methods have failed to produce significant results. The primary goal of bariatric surgery is to reduce the size of the stomach and/or alter the digestive process, leading to weight loss and improvement or resolution of obesity-related health conditions.
There are several types of bariatric surgery procedures, each with its own mechanisms of action and effects on weight loss. Some common types include:
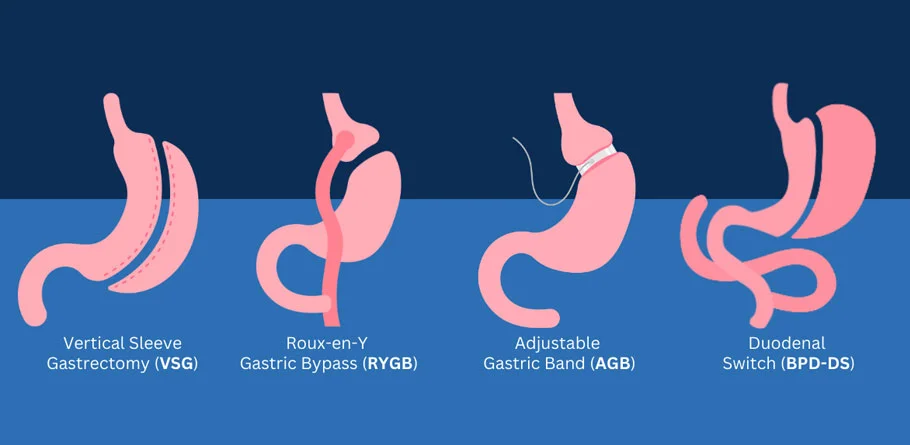
- Gastric Bypass Surgery (Roux-en-Y Gastric Bypass): This procedure involves creating a small pouch at the top of the stomach and connecting it directly to the small intestine, bypassing a portion of the stomach and the first part of the small intestine. This reduces the amount of food the stomach can hold and limits the absorption of calories and nutrients.
- Sleeve Gastrectomy: In this procedure, a portion of the stomach is removed, leaving a smaller sleeve-shaped stomach. This reduces the stomach's capacity, leading to earlier feelings of fullness and reduced food intake.
- Adjustable Gastric Banding (Lap-Band): A band is placed around the upper part of the stomach to create a small pouch, restricting the amount of food that can be consumed at one time. The band can be adjusted to control the size of the opening between the pouch and the rest of the stomach.
- Biliopancreatic Diversion with Duodenal Switch (BPD/DS): This procedure combines aspects of gastric bypass and sleeve gastrectomy. It involves removing a portion of the stomach and rerouting the small intestine to limit both food intake and nutrient absorption.
Candidates for bariatric surgery typically have a body mass index (BMI) of 40 or higher, or a BMI of 35 or higher with obesity-related health conditions such as type 2 diabetes, high blood pressure, or sleep apnea. The decision to undergo bariatric surgery is made after a thorough evaluation by a multidisciplinary team, including a surgeon, dietitian, psychologist, and other healthcare professionals.
Bariatric surgery is not a quick fix for obesity, but rather a tool to assist with weight loss and improve overall health. Patients are required to make significant lifestyle changes, including adopting a healthier diet and incorporating regular exercise, to achieve and maintain successful weight loss after surgery.
Retroperitoneal Tumours
Retroperitoneal Tumours
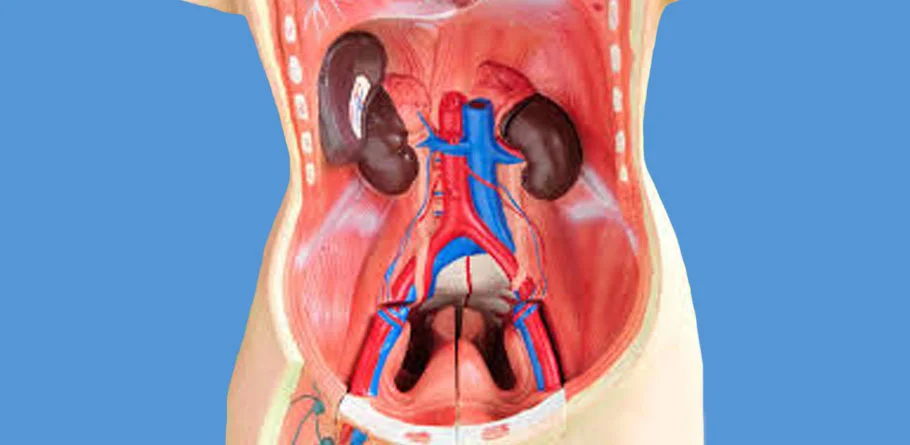
Retroperitoneal tumors are abnormal growths that develop in the retroperitoneal space, which is the area located behind the peritoneum (the membrane lining the abdominal cavity) and in front of the spine. These tumors can arise from various types of tissues, including fat cells, connective tissue, nerve cells, blood vessels, and organs such as the kidneys and adrenal glands.
These tumors are relatively rare and can be benign (non-cancerous) or malignant (cancerous). Malignant retroperitoneal tumors are more common than benign ones. The symptoms of retroperitoneal tumors can vary depending on their size, location, and whether they are benign or malignant. Common symptoms may include:
- Abdominal or back pain: Pain may be dull or sharp and may worsen over time.
- Abdominal mass or swelling: A palpable lump may be felt in the abdomen.
- Weight loss: Unexplained weight loss may occur in some cases.
- Changes in bowel or bladder habits: This may include constipation, diarrhea, or difficulty urinating.
- Nausea and vomiting: These symptoms may occur if the tumor is pressing on the stomach or intestines.
Diagnosis of retroperitoneal tumors typically involves a combination of imaging studies such as computed tomography (CT) scans, magnetic resonance imaging (MRI), and ultrasound. Biopsy may also be performed to determine the nature of the tumor (benign or malignant).
Treatment options for retroperitoneal tumors depend on various factors including the type of tumor, its size, location, and whether it is benign or malignant. Treatment may involve:
- Surgery: Surgical removal of the tumor is often the primary treatment for retroperitoneal tumors, especially if they are malignant or causing symptoms. The goal of surgery is to remove the entire tumor while preserving nearby organs and structures as much as possible.
- Chemotherapy: Chemotherapy may be recommended for malignant retroperitoneal tumors, either before surgery (neoadjuvant chemotherapy) to shrink the tumor or after surgery (adjuvant chemotherapy) to kill any remaining cancer cells.
- Radiation therapy: Radiation therapy may be used in combination with surgery and/or chemotherapy to treat retroperitoneal tumors, particularly if they cannot be completely removed surgically or if there is a risk of recurrence.
- Observation: In some cases, especially for small, slow-growing benign tumors that are not causing symptoms, a watch-and-wait approach may be recommended, with regular monitoring to check for any changes in the tumor.
Cancer Surgeries
Esophagus
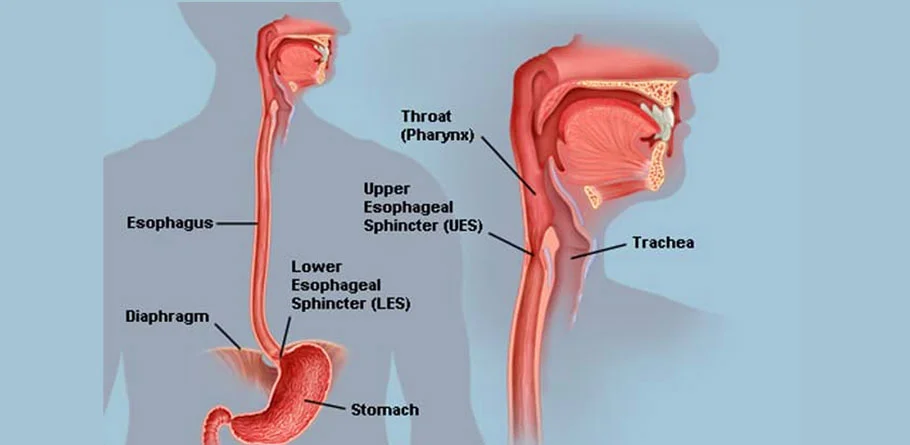
The esophagus is a muscular tube that connects the throat (pharynx) with the stomach. Its primary function is to transport food and liquids from the mouth to the stomach for digestion. The esophagus is located in the upper chest and runs behind the windpipe (trachea) and in front of the spine.
- Muscular Structure: The walls of the esophagus are made up of layers of smooth muscle tissue that contract and relax in a coordinated manner to propel food downward toward the stomach. This process, known as peristalsis, helps facilitate swallowing.
- Mucosal Lining: The inner lining of the esophagus is composed of mucous membrane tissue, which secretes mucus to lubricate the passage of food and protect the esophageal walls from damage caused by stomach acid and digestive enzymes.
- Lower Esophageal Sphincter (LES): At the junction between the esophagus and the stomach, there is a specialized ring of muscle called the lower esophageal sphincter. This sphincter opens to allow food to enter the stomach and then closes to prevent stomach contents, including acid, from flowing back up into the esophagus. Dysfunction of the LES can lead to gastroesophageal reflux disease (GERD), a condition characterized by acid reflux and heartburn.
- Upper Esophageal Sphincter (UES): At the upper end of the esophagus, there is another muscular ring known as the upper esophageal sphincter. This sphincter helps prevent air from entering the esophagus during breathing and keeps swallowed food and liquids from regurgitating back into the throat.
- Epithelial Cells: The mucosal lining of the esophagus is made up of stratified squamous epithelial cells, which provide protection against abrasion and mechanical damage from food particles as they pass through the esophagus.
Disorders and conditions that can affect the esophagus include:
- Gastroesophageal reflux disease (GERD)
- Esophagitis (inflammation of the esophagus)
- Esophageal strictures (narrowing of the esophagus)
- Esophageal cancer
- Esophageal motility disorders (e.g., achalasia)
- Barrett's esophagus (a condition in which the normal tissue lining the esophagus is replaced by tissue similar to the lining of the intestine)

Stomach
The stomach is a muscular organ located in the upper abdomen, just below the rib cage, on the left side of the body. Its primary function is to store, digest, and break down food that has been ingested before it is further processed in the small intestine. The stomach plays a crucial role in the digestive process by secreting gastric juices containing acids and enzymes necessary for the breakdown of food molecules.
- Gastric Lining: The inner lining of the stomach is composed of specialized cells that secrete gastric juices, including hydrochloric acid (HCl) and digestive enzymes such as pepsin. These substances help break down proteins, fats, and carbohydrates into smaller molecules that can be absorbed in the intestines.
- Mucous Cells: The stomach also contains mucous-secreting cells that produce a thick layer of mucus, which coats the stomach lining and protects it from the corrosive effects of gastric acid.
- Muscular Layers: The walls of the stomach are made up of three layers of smooth muscle tissue arranged in longitudinal, circular, and oblique orientations. These muscles contract and relax in a coordinated manner to churn and mix food with gastric juices, forming a semi-liquid substance known as chyme.
- Sphincters: The stomach is connected to the esophagus by the lower esophageal sphincter (LES), which opens to allow food to enter the stomach and then closes to prevent the backflow of stomach contents into the esophagus. At the lower end of the stomach, there is another muscular ring called the pyloric sphincter, which regulates the passage of chyme from the stomach into the small intestine.
- Gastric Emptying: Once food has been sufficiently processed in the stomach, it is gradually emptied into the small intestine through the pyloric sphincter. Gastric emptying is controlled by various factors including the volume and composition of the meal, the presence of hormones and neural signals, and the contraction of stomach muscles.
Disorders and conditions that can affect the stomach include:
- Gastritis (inflammation of the stomach lining)
- Peptic ulcers (open sores in the stomach lining)
- Gastroenteritis (stomach flu)
- Gastric cancer
- Gastroparesis (delayed stomach emptying)
- Gastroesophageal reflux disease (GERD)
- Helicobacter pylori infection (bacterial infection associated with peptic ulcers)
Small Intestine
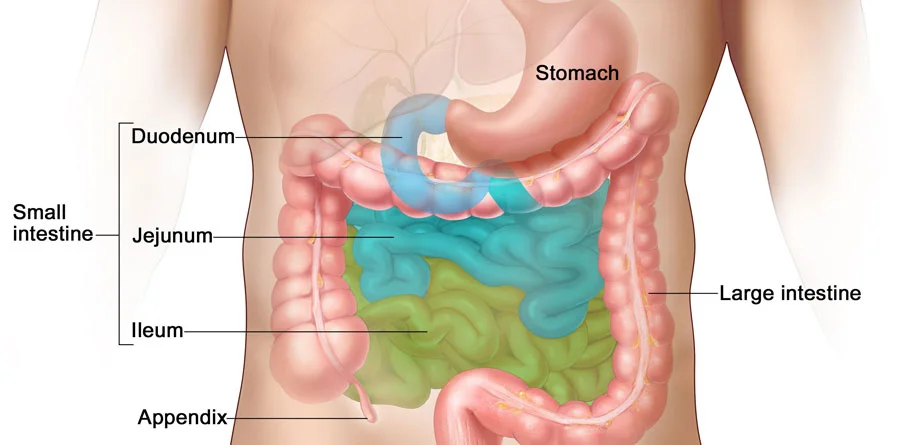
The small intestine is a vital part of the digestive system, located between the stomach and the large intestine. It is where most of the digestion and absorption of nutrients from food occurs. Despite its name, the small intestine is actually the longest part of the digestive tract in humans, measuring around 20 feet (6 meters) in length.
- Three Segments: The small intestine is divided into three main segments: the duodenum, the jejunum, and the ileum. The duodenum is the shortest segment and is primarily responsible for receiving partially digested food from the stomach, as well as digestive juices from the pancreas and bile from the liver. The jejunum and ileum make up the remaining length of the small intestine and are primarily involved in nutrient absorption.
- Intestinal Villi and Microvilli: The lining of the small intestine is covered in tiny finger-like projections called villi, which greatly increase the surface area available for absorption. Each villus contains even smaller projections called microvilli, further increasing the absorptive surface area. Together, the villi and microvilli provide an extensive surface area for the absorption of nutrients such as carbohydrates, proteins, fats, vitamins, and minerals into the bloodstream.
- Digestive Enzymes: The small intestine secretes various enzymes and digestive juices to further break down food molecules into smaller components that can be absorbed. Enzymes produced by the pancreas, such as amylase, lipase, and proteases, help digest carbohydrates, fats, and proteins, respectively. Bile, produced by the liver and stored in the gallbladder, aids in the digestion and absorption of fats.
- Peristalsis: Like the rest of the digestive tract, the small intestine undergoes rhythmic contractions known as peristalsis, which propel food and chyme (partially digested food) through its length. Peristalsis helps mix the chyme with digestive juices and facilitates nutrient absorption.
- Absorption of Nutrients: The small intestine is the primary site of nutrient absorption in the digestive system. Nutrients are absorbed across the epithelial cells lining the intestinal villi and are then transported into the bloodstream or lymphatic system for distribution to cells throughout the body
- Water Absorption: In addition to nutrient absorption, the small intestine also plays a role in absorbing water and electrolytes from the digestive tract, helping to maintain fluid balance in the body.

Colon Cancer
Colon cancer, also known as colorectal cancer, is a type of cancer that starts in the colon or rectum, which are parts of the large intestine. It usually begins as a small growth called a polyp, which may or may not be cancerous. Over time, some polyps can develop into cancer.
- Risk Factors: Several factors can increase the risk of developing colon cancer, including age (risk increases with age), a personal or family history of colon cancer or polyps, inflammatory bowel diseases such as Crohn's disease or ulcerative colitis, a diet high in red and processed meats, obesity, smoking, heavy alcohol consumption, and a sedentary lifestyle.
- Symptoms: Early-stage colon cancer often does not cause symptoms, which is why screening is crucial for early detection. As the cancer progresses, symptoms may include changes in bowel habits (such as diarrhea, constipation, or narrowing of the stool), rectal bleeding or blood in the stool, abdominal discomfort or pain, unexplained weight loss, weakness or fatigue, and a feeling that the bowel does not empty completely.
- Diagnosis: Diagnosis of colon cancer typically involves a combination of screening tests and diagnostic procedures. Common screening methods include colonoscopy, fecal occult blood tests (FOBT), fecal immunochemical tests (FIT), and stool DNA tests. If abnormalities are detected during screening, further diagnostic tests such as colonoscopy with biopsy, imaging studies (e.g., CT scan, MRI), and blood tests may be performed to confirm the diagnosis and determine the extent of the cancer.
- Treatment: Treatment for colon cancer depends on several factors including the stage of the cancer, its location, and the overall health of the patient. Common treatment options may include surgery to remove the cancerous tissue (often along with nearby lymph nodes), chemotherapy, radiation therapy, targeted therapy, and immunotherapy. In some cases, a combination of these treatments may be recommended.
- Prognosis: The prognosis for colon cancer varies depending on the stage at which it is diagnosed and treated. Early-stage colon cancer that is confined to the inner layers of the colon or rectum generally has a better prognosis than cancer that has spread to nearby lymph nodes or distant organs. Regular screening can help detect colon cancer at an early stage when treatment is most effective.
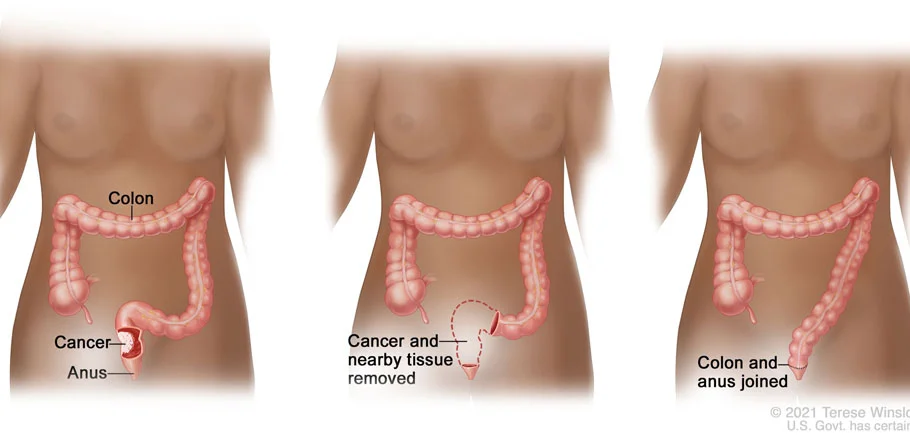
Rectum
Surgery is a primary treatment for rectal cancer, aimed at removing the cancerous tissue and, if necessary, nearby lymph nodes. The type of surgery performed for rectal cancer depends on several factors, including the stage and location of the cancer, as well as the patient's overall health. Here are some common surgical procedures used in the treatment of rectal cancer:
- Transanal Excision (TAE): This procedure is typically used for small, early-stage rectal cancers that are located close to the anus. During a transanal excision, the cancerous tissue is removed through the anus using specialized instruments. TAE is a minimally invasive approach that may be performed under local anesthesia.
- Transanal Endoscopic Microsurgery (TEM): Similar to TAE, TEM is used for early-stage rectal cancers near the anus. However, TEM utilizes specialized equipment, including an endoscope and microscope, to provide better visualization and precision during surgery.
- Low Anterior Resection (LAR): LAR is a surgical procedure used to remove the cancerous tissue in the upper part of the rectum while preserving the anus and sphincter muscles. After removing the cancerous portion of the rectum, the remaining healthy tissue is reattached to the colon, allowing for normal bowel function.
- Abdominoperineal Resection (APR): APR is performed for rectal cancers located very close to the anus or in the lower part of the rectum. During an APR, the entire rectum, anus, and surrounding tissues are removed. After the rectum is removed, the surgeon creates a permanent colostomy, where the end of the colon is brought out through an opening in the abdomen (stoma), allowing waste to exit the body into a pouch worn outside the body.
- Total Mesorectal Excision (TME): TME is a meticulous surgical technique used to remove the rectum and surrounding lymph nodes while preserving the nerves that control bowel and bladder function. TME aims to achieve complete removal of the cancerous tissue while minimizing damage to nearby structures.
Surgery for Hydatid Cyst of Liver
Surgery for Hydatid Cyst of Liver
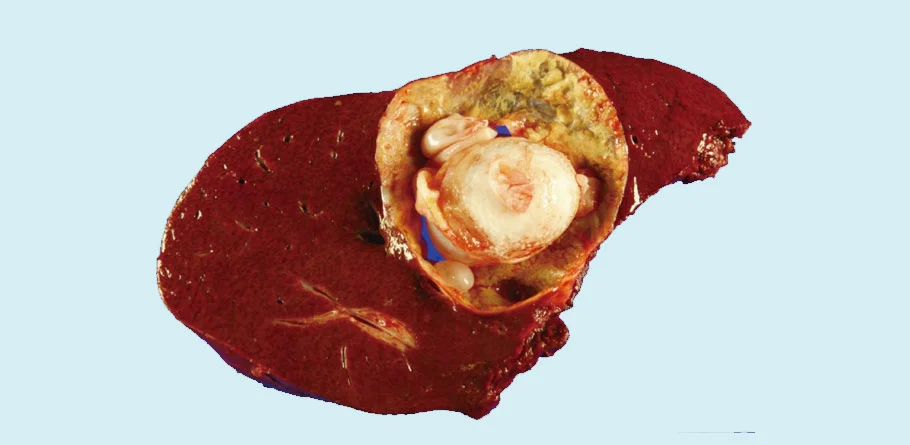
Surgery is often the primary treatment for hydatid cysts of the liver, which are caused by infection with the parasitic tapeworm Echinococcus granulosus. Hydatid cysts can cause symptoms such as abdominal pain, nausea, vomiting, jaundice, and fever, and if left untreated, they can lead to complications such as cyst rupture, infection, and obstruction of nearby organs.
The surgical approach to treating hydatid cysts of the liver depends on several factors, including the size, location, and number of cysts, as well as the overall health of the patient. Here are some common surgical options for hydatid cysts of the liver:
- Cystectomy: In cases where the hydatid cyst is small and located in a favorable position within the liver, a cystectomy may be performed. During a cystectomy, the surgeon removes the entire cyst while preserving as much healthy liver tissue as possible.
- Partial Hepatectomy: If the hydatid cyst is large or located near the surface of the liver, a partial hepatectomy may be necessary. This involves removing a portion of the liver containing the cyst while preserving the remaining liver tissue. The extent of liver resection depends on the size and location of the cyst.
- Percutaneous Aspiration, Injection, and Reaspiration (PAIR): In some cases, particularly for cysts that are difficult to access surgically or for patients who are not suitable candidates for surgery, a minimally invasive procedure known as PAIR may be performed. During PAIR, the cyst is punctured using a needle, and the fluid is aspirated. Then, a scolicidal agent (a substance that kills the parasitic larvae) is injected into the cyst, followed by reaspiration of the fluid. PAIR is often used as an adjunct to surgery or as a primary treatment for small cysts.
- Hydatid Cystectomy with Omentoplasty: In cases where the hydatid cyst has ruptured or is densely adherent to surrounding tissues, a more extensive surgical procedure known as cystectomy with omentoplasty may be necessary. This involves removing the entire cyst along with surrounding tissue, followed by the placement of a flap of omentum (a fold of tissue from the lining of the abdomen) over the residual cavity to prevent recurrence and promote healing.
- Laparoscopic Surgery: In select cases, laparoscopic or minimally invasive surgical techniques may be used to remove hydatid cysts of the liver. These procedures involve making small incisions in the abdomen and using specialized instruments and a camera to visualize and remove the cysts. Laparoscopic surgery may offer benefits such as shorter hospital stays, faster recovery, and reduced postoperative pain compared to traditional open surgery.
Cancer Surgeries
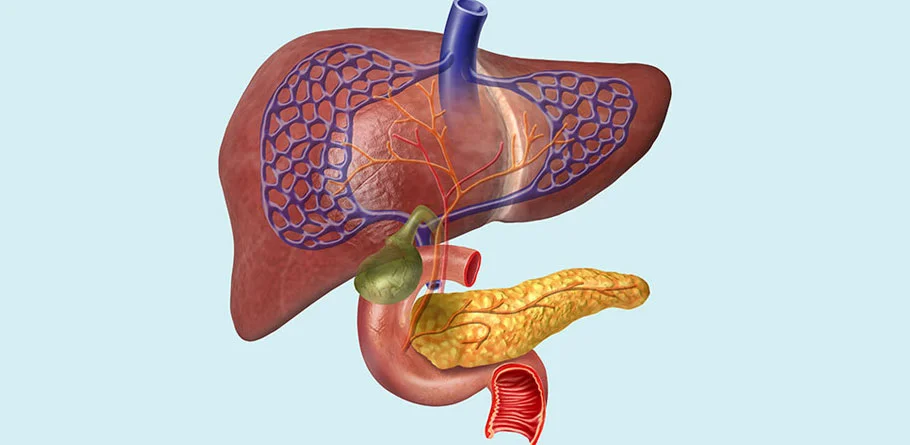
Liver
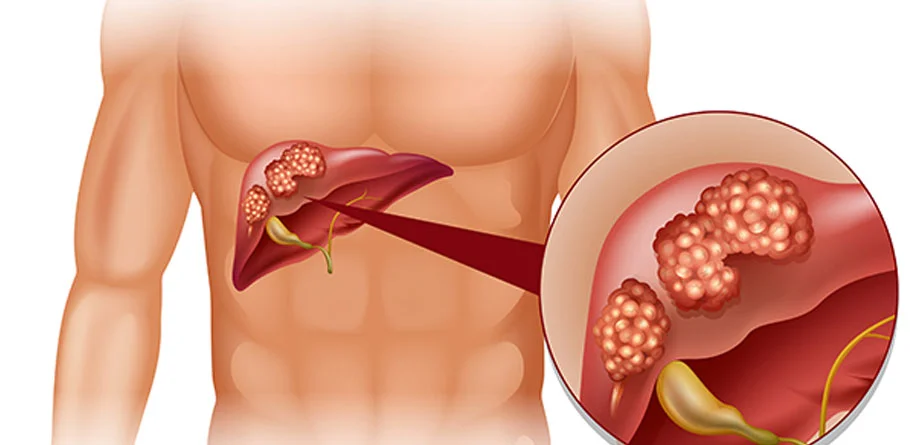
Liver cancer, particularly hepatocellular carcinoma (HCC) and intrahepatic cholangiocarcinoma (ICC), falls under the category of hepatopancreatobiliary (HPB) cancers. Surgical intervention plays a crucial role in the management of liver HPB cancers, aiming to remove the tumor and potentially cure the disease, particularly in early-stage cases. Various surgical procedures may be employed based on the extent of the cancer, liver function, and overall health of the patient.
Liver Resection:
- Liver resection, also known as partial hepatectomy, involves the surgical removal of a portion of the liver containing the cancerous tumor. This procedure is suitable for patients with localized liver cancer and sufficient remaining liver tissue to maintain adequate liver function post-surgery.
- The goal of liver resection is to achieve complete removal of the tumor while preserving as much healthy liver tissue as possible. The extent of resection depends on the size, location, and number of tumors, as well as the underlying liver function.
- Advances in surgical techniques, including minimally invasive approaches such as laparoscopic or robotic-assisted liver resection, have improved outcomes and reduced postoperative complications for eligible patients.
Locoregional Transplantation
- Liver transplantation may be considered for select patients with early-stage liver cancer who meet specific criteria, such as limited tumor size and number, absence of vascular invasion or extrahepatic spread, and adequate liver function.
- During liver transplantation, the entire diseased liver is removed and replaced with a healthy donor liver. This procedure offers the potential for cure and can be particularly beneficial for patients with underlying liver disease, such as cirrhosis, who are at high risk of tumor recurrence after resection.
Locoregional Therapies:
- In addition to surgery, locoregional therapies such as radiofrequency ablation (RFA), microwave ablation (MWA), transarterial chemoembolization (TACE), and selective internal radiation therapy (SIRT) may be used to treat unresectable liver tumors or as adjunctive therapies to surgery.
- These minimally invasive procedures aim to destroy cancerous tissue within the liver while sparing healthy surrounding tissue, providing options for patients who are not candidates for surgery or liver transplantation.
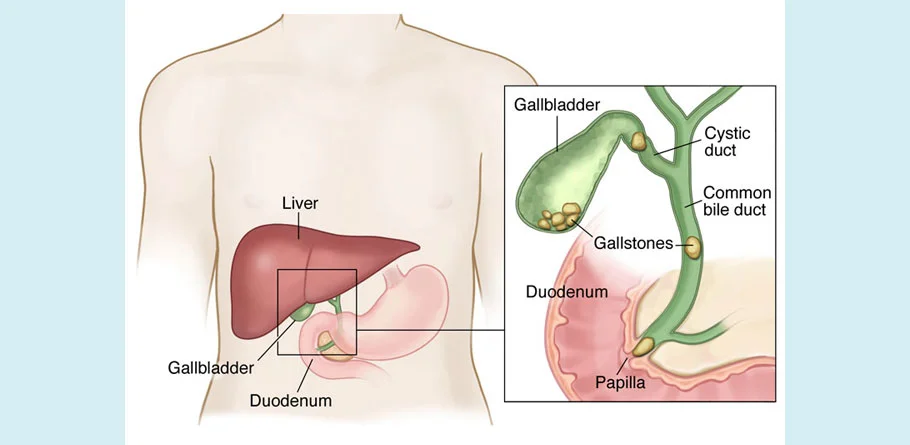
Gall Bladder
The gallbladder is a small, pear-shaped organ located beneath the liver in the upper right abdomen. It plays a crucial role in the digestive process by storing and concentrating bile, a fluid produced by the liver that helps in the digestion and absorption of fats in the small intestine. The gallbladder releases bile into the small intestine in response to the ingestion of fatty foods.
- Bile Storage and Concentration: The primary function of the gallbladder is to store and concentrate bile produced by the liver. Bile is composed of water, bile salts, cholesterol, and bilirubin, among other substances. When bile is not needed for digestion, it is stored and concentrated in the gallbladder, which helps to increase its potency.
- Bile Release: When fatty foods enter the small intestine during a meal, hormonal signals stimulate the gallbladder to contract and release bile into the small intestine through the bile duct. Bile aids in the digestion and absorption of fats by emulsifying them into smaller droplets, which increases the surface area for digestive enzymes to act upon.
- Gallstones: Gallstones are hardened deposits that can form in the gallbladder due to an imbalance in the components of bile, such as cholesterol or bilirubin. Gallstones can vary in size and may cause symptoms such as abdominal pain, nausea, vomiting, and jaundice if they block the flow of bile from the gallbladder. In some cases, gallstones may require medical treatment or surgical removal of the gallbladder (cholecystectomy).
- Cholecystectomy: Cholecystectomy is a surgical procedure used to remove the gallbladder, typically when it becomes inflamed, infected, or when gallstones cause symptoms. Cholecystectomy is one of the most common surgical procedures performed in the United States. Most cholecystectomies are performed using minimally invasive techniques such as laparoscopic surgery, which involves making several small incisions in the abdomen and using specialized instruments to remove the gallbladder.
- Biliary System: The gallbladder is part of the biliary system, which also includes the liver, bile ducts, and pancreas. Bile produced by the liver is transported through the bile ducts to the gallbladder for storage and concentration. After meals, bile is released from the gallbladder into the small intestine to aid in digestion.
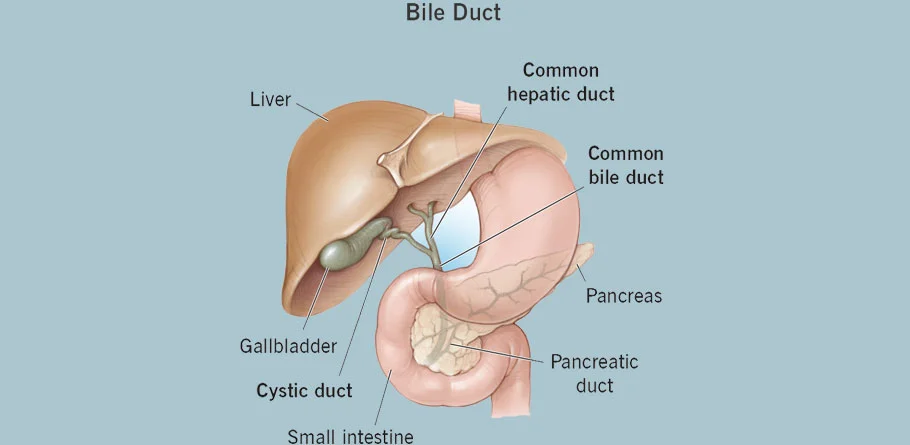
Bile Duct
Bile duct cancer, also known as cholangiocarcinoma, is a rare but aggressive type of cancer that affects the bile ducts, which are the tubes that carry bile from the liver and gallbladder to the small intestine. Surgery is often a key component of treatment for bile duct cancer, particularly for early-stage tumors or cases where the cancer is localized and operable. The specific surgical procedure performed depends on several factors, including the location and extent of the cancer, as well as the patient's overall health. Here are some common surgical options for bile duct cancer:
- Partial Hepatectomy: This procedure involves removing a portion of the liver along with the tumor if the cancer is located in the bile ducts within the liver (intrahepatic bile ducts). The extent of liver tissue removed depends on the size and location of the tumor.
- Whipple Procedure (Pancreaticoduodenectomy): The Whipple procedure is a complex surgery performed for tumors located in the common bile duct, where it passes through the head of the pancreas. During this procedure, the surgeon removes the head of the pancreas, the first part of the small intestine (duodenum), the gallbladder, part of the bile duct, and sometimes a portion of the stomach. The remaining structures are then reconstructed to restore the flow of bile and digestive juices.
- Extrahepatic Bile Duct Resection (Bile Duct Excision): If the cancer is confined to the bile duct outside the liver (extrahepatic bile ducts), a surgical procedure known as extrahepatic bile duct resection may be performed. This involves removing the segment of the bile duct containing the tumor, as well as nearby lymph nodes.
- Liver Transplantation: In some cases of bile duct cancer that cannot be removed by standard surgical techniques, liver transplantation may be considered as a treatment option. This is more commonly performed for intrahepatic bile duct cancers.
- Palliative Surgery: For advanced cases of bile duct cancer that cannot be completely removed, palliative surgery may be performed to relieve symptoms and improve quality of life. This may involve procedures such as placing stents to keep the bile duct open and alleviate bile duct blockage, or bypass surgery to reroute bile flow around the blocked area.

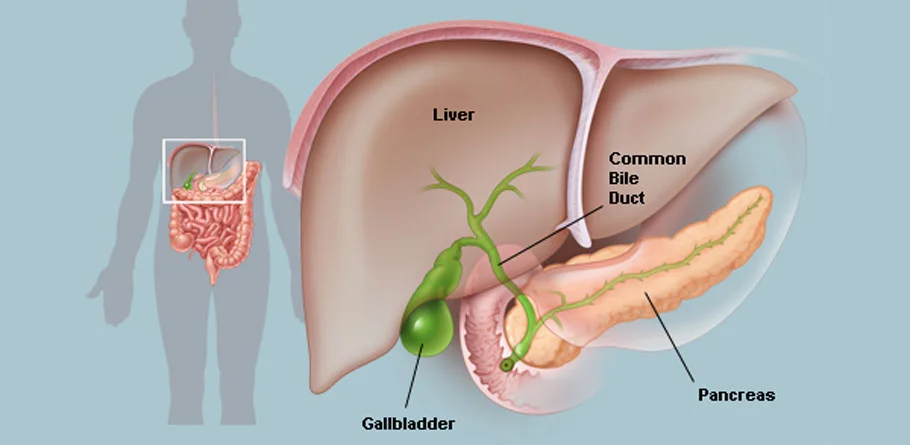
Pancreas
Pancreatic cancer, including cancers of the hepatobiliary (HPB) system (which includes the liver and bile ducts), often requires surgery as part of its treatment plan. The type of surgery performed depends on various factors, including the location and stage of the cancer, as well as the patient's overall health. Here are some common surgical options for pancreatic and HPB cancers: The surgical approach to treating hydatid cysts of the liver depends on several factors, including the size, location, and number of cysts, as well as the overall health of the patient. Here are some common surgical options for hydatid cysts of the liver:
- Pancreaticoduodenectomy (Whipple Procedure): This is the most common surgery for cancers located in the head of the pancreas, ampulla of Vater, or periampullary region. During the Whipple procedure, the surgeon removes the head of the pancreas, the first part of the small intestine (duodenum), the gallbladder, the bile duct, and sometimes a portion of the stomach. The remaining structures are then reconstructed to restore the flow of bile and digestive juices.
- Distal Pancreatectomy: This surgery involves removing the tail and sometimes part of the body of the pancreas. It is typically performed for cancers located in the body or tail of the pancreas.
- Total Pancreatectomy: In rare cases where the cancer involves the entire pancreas, a total pancreatectomy may be performed. This surgery involves removing the entire pancreas, as well as the spleen and portions of the stomach, small intestine, and bile duct.
- Liver Resection (Hepatectomy): If the cancer has spread to the liver, surgery to remove part of the liver (liver resection or hepatectomy) may be performed. The extent of liver resection depends on the size, location, and number of tumors.
- Bile Duct Resection (Hepatectomy with Bile Duct Resection): For cancers involving the bile ducts (cholangiocarcinoma), surgical resection of the affected bile duct segment along with nearby liver tissue and lymph nodes may be performed.
- Palliative Surgery: In cases where the cancer is advanced and cannot be completely removed, palliative surgery may be performed to relieve symptoms and improve quality of life. This may involve procedures such as placing stents to keep bile ducts or the duodenum open and alleviate blockages caused by the tumor.
Emergency Laparotomy
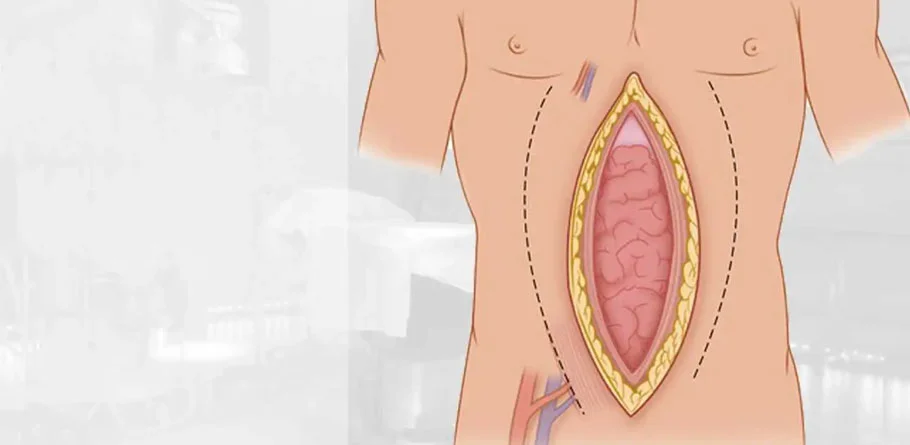
Emergency Laparotomy
An emergency laparotomy is a life-saving surgical procedure performed urgently to address critical abdominal conditions requiring immediate intervention. It serves as a vital tool in the armamentarium of surgeons for diagnosing and treating a wide range of acute abdominal emergencies, ranging from traumatic injuries to acute abdominal conditions and visceral vascular emergencies.
In the context of trauma, an emergency laparotomy may be required to address abdominal injuries resulting from blunt or penetrating trauma. Such injuries can lead to internal bleeding, organ damage, or perforation of the bowel, necessitating prompt surgical exploration and intervention to control bleeding, repair injuries, and prevent further complications. This timely intervention can be crucial in stabilizing patients and improving their chances of survival.
Acute abdominal conditions such as appendicitis, intestinal obstruction, perforated ulcers, and mesenteric ischemia can also necessitate emergency laparotomy. These conditions often present with severe abdominal pain, signs of peritonitis, or other life-threatening complications requiring immediate surgical assessment and management. Through surgical exploration, the underlying cause can be identified and addressed, whether it involves removing inflamed or necrotic tissue, relieving obstructions, or restoring blood flow to ischemic organs.
Abdominal infections, including peritonitis and intra-abdominal abscesses, represent another category of emergencies warranting urgent surgical intervention. Emergency laparotomy allows for drainage of infected fluid, removal of necrotic tissue, and administration of antibiotics to combat the infection and prevent systemic complications.
Gastrointestinal bleeding, whether from ulcers, tumors, or vascular abnormalities, can result in massive hemorrhage necessitating emergency laparotomy to identify and control the bleeding source. The surgical approach may involve hemostasis techniques, ligation of bleeding vessels, or resection of diseased tissue to achieve hemodynamic stability and prevent further blood loss. General Surgery Emergency Laparotomy Gall bladder Stones CBD Stones Appendix Hernia Lipoma/ Sebaceous Cyst Hydrocoele Circumcision Piles/ Fissures Abscess Drainage Debridement (Bedsores, Diabetic Foot) Call Us (+91) 9920766648 Mail Us rohaangazdar@gmail.com Mail Us
Gall bladder Stones

Gall bladder Stones
Gallstones are solid particles that form in the gallbladder, a small organ located beneath the liver. These stones develop when the components of bile, a digestive fluid produced by the liver and stored in the gallbladder, become imbalanced. The primary constituents of gallstones are cholesterol, bilirubin, and calcium salts. Gallstones can vary in size, ranging from as small as a grain of sand to as large as a golf ball, and individuals can have a single stone or multiple stones in their gallbladder.
While many people with gallstones may not experience symptoms, they can cause discomfort and complications when they obstruct the flow of bile or become lodged in the bile ducts. Symptoms of gallstones may include biliary colic, characterized by sudden and intense pain in the upper abdomen or right side, nausea, vomiting, abdominal discomfort, and jaundice (yellowing of the skin and eyes).
Complications associated with gallstones can include cholecystitis (inflammation of the gallbladder), choledocholithiasis (blockage of the bile ducts), pancreatitis (inflammation of the pancreas), and cholangitis (infection of the bile ducts). Diagnosis of gallstones is typically made through imaging tests such as ultrasound, which can visualize the gallbladder and detect the presence of stones.
Treatment for gallstones depends on the presence of symptoms and complications. In cases where gallstones are causing symptoms or complications, the most common treatment is cholecystectomy, the surgical removal of the gallbladder. This procedure is usually performed laparoscopically and is highly effective in relieving symptoms and preventing recurrence. In some cases, medications may be prescribed to dissolve cholesterol gallstones, but they are not effective for all types of stones and may take months or years to be successful.
CBD Stones
CBD Stones
Common bile duct (CBD) stones, also known as choledocholithiasis, are solid particles that form in the common bile duct, which is the duct that carries bile from the liver and gallbladder to the small intestine. These stones typically originate in the gallbladder and migrate into the common bile duct, where they can cause obstruction, inflammation, and other complications.
CBD stones are primarily composed of cholesterol or bilirubin, similar to gallstones, and they can vary in size from small particles to larger stones that may completely obstruct the bile duct. The presence of CBD stones can lead to symptoms such as jaundice (yellowing of the skin and eyes), abdominal pain, nausea, vomiting, fever, and dark urine.
The risk factors for developing CBD stones are similar to those for gallstones and include factors such as obesity, a high-fat diet, rapid weight loss, and certain medical conditions such as liver cirrhosis or inflammatory bowel disease.
Diagnosis of CBD stones typically involves imaging tests such as ultrasound, computed tomography (CT) scan, magnetic resonance cholangiopancreatography (MRCP), or endoscopic retrograde cholangiopancreatography (ERCP). These tests can visualize the bile ducts and detect the presence of stones.
Appendix
Appendix
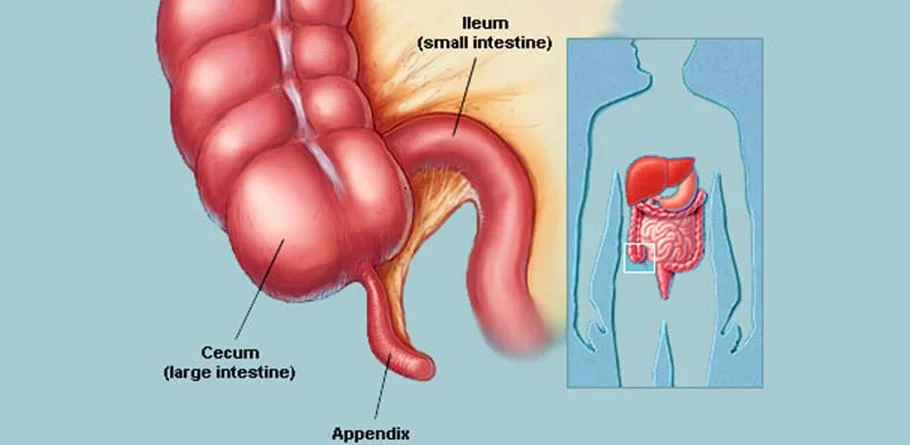
The appendix is a small, finger-shaped pouch attached to the large intestine, specifically to the cecum, which is the beginning of the large intestine. Positioned in the lower right abdomen, the appendix has long been considered a vestigial organ, meaning it serves no apparent purpose in humans. However, recent research suggests that the appendix may play a role in the immune system, specifically in the storage of beneficial gut bacteria.
Despite its unclear function, the appendix can become inflamed and infected, a condition known as appendicitis. Appendicitis occurs when the opening of the appendix becomes blocked, usually by a small piece of stool, a foreign body, or, in some cases, by a tumor. The blockage can lead to bacterial overgrowth, inflammation, and swelling of the appendix. If left untreated, appendicitis can progress to a ruptured appendix, a potentially life-threatening condition that can lead to severe infection of the abdominal cavity.
Symptoms of appendicitis typically include:
- Abdominal Pain: The most common symptom of appendicitis is abdominal pain that starts around the belly button and then moves to the lower right abdomen. The pain may worsen with movement, coughing, or deep breathing.
- Loss of Appetite: Many people with appendicitis experience a loss of appetite and may feel nauseous or vomit.
- Fever and Chills: Appendicitis can cause fever and chills, especially if the appendix becomes infected.
- Changes in Bowel Habits: Some individuals may experience changes in bowel habits, such as diarrhea or constipation.
Diagnosis of appendicitis typically involves a physical examination, blood tests, and imaging studies such as ultrasound or computed tomography (CT) scan. Treatment usually involves surgical removal of the appendix, a procedure known as appendectomy. Appendectomy is often performed laparoscopically, using small incisions and a camera to guide the surgeon. In some cases, an open appendectomy may be necessary, particularly if the appendix has ruptured or if laparoscopic surgery is not feasible.
Hernia

Hernia
A hernia occurs when an organ or tissue protrudes through a weak spot or opening in the surrounding muscle or connective tissue that normally holds it in place. Hernias can develop in various parts of the body, but they most commonly occur in the abdomen, particularly in areas where there is a natural weakness or potential for strain.
There are several types of hernias, including:
- Inguinal Hernia: This is the most common type of hernia and occurs when part of the intestine protrudes through a weak spot in the abdominal wall near the groin. Inguinal hernias are more common in men and may cause a bulge or swelling in the groin area.
- Femoral Hernia: Similar to inguinal hernias, femoral hernias also occur in the groin area but are less common. They occur when tissue protrudes through the femoral canal, a passageway near the groin.
- Hiatal Hernia: This type of hernia occurs when part of the stomach protrudes through the diaphragm into the chest cavity. Hiatal hernias can cause symptoms such as heartburn, chest pain, and difficulty swallowing.
- Umbilical Hernia: Umbilical hernias occur when part of the intestine protrudes through the abdominal wall near the belly button (umbilicus). They are more common in infants but can also occur in adults, particularly in women who have been pregnant.
- Incisional Hernia: This type of hernia occurs at the site of a previous abdominal surgery where the abdominal muscles have weakened, allowing tissue to protrude through the scar tissue.
Risk factors for hernias include age, gender (men are more prone to inguinal hernias), obesity, pregnancy, chronic coughing or straining (such as from heavy lifting or constipation), and certain medical conditions that increase intra-abdominal pressure.
Symptoms of a hernia may vary depending on the type and location but commonly include a visible bulge or swelling, discomfort or pain, especially when lifting or bending over, and a feeling of heaviness or pressure in the affected area.
Lipoma/ Sebaceous Cyst

Lipoma/ Sebaceous Cyst
Lipomas and sebaceous cysts are two common types of benign skin growths that can occur anywhere on the body. While they may share some similarities, they arise from different types of tissue and have distinct characteristics.
Lipoma:
- Lipomas are soft, rubbery, movable lumps that develop beneath the skin. They are composed of fatty tissue and typically feel doughy or squishy to the touch.
- These growths are usually painless and slow-growing, and they can vary in size from small pea-sized nodules to larger masses several inches in diameter.
- Lipomas are most commonly found on the neck, shoulders, back, abdomen, or thighs, but they can occur anywhere on the body where fat cells are present.
- While the exact cause of lipomas is unknown, they may develop due to genetic factors, hormonal imbalances, or trauma to the affected area.
- Lipomas are generally harmless and do not require treatment unless they cause discomfort, interfere with movement, or are of cosmetic concern. Surgical removal (excision) is the most common treatment option and is usually performed as an outpatient procedure under local anesthesia.
Sebaceous Cyst:
- Sebaceous cysts, also known as epidermoid cysts, are noncancerous growths that develop beneath the skin's surface. They are typically filled with keratin, a protein found in skin cells, and sebum, an oily substance produced by the skin's oil glands.
- Sebaceous cysts often present as round, firm, or movable lumps that may feel smooth or have a dome-like appearance on the skin's surface.
- These cysts commonly occur on the face, neck, scalp, back, or genitals, where hair follicles and oil glands are abundant.
- The exact cause of sebaceous cysts is not always clear, but they may develop due to blocked hair follicles, trauma to the skin, or underlying skin conditions.
- Sebaceous cysts are usually harmless and asymptomatic unless they become infected, inflamed, or rupture, causing pain, redness, and drainage of thick, foul-smelling fluid.
- Treatment for sebaceous cysts may include drainage of the cyst's contents, injection of corticosteroids to reduce inflammation, or surgical excision if the cyst is large, symptomatic, or prone to recurrence.
Hydrocoele
Hydrocoele
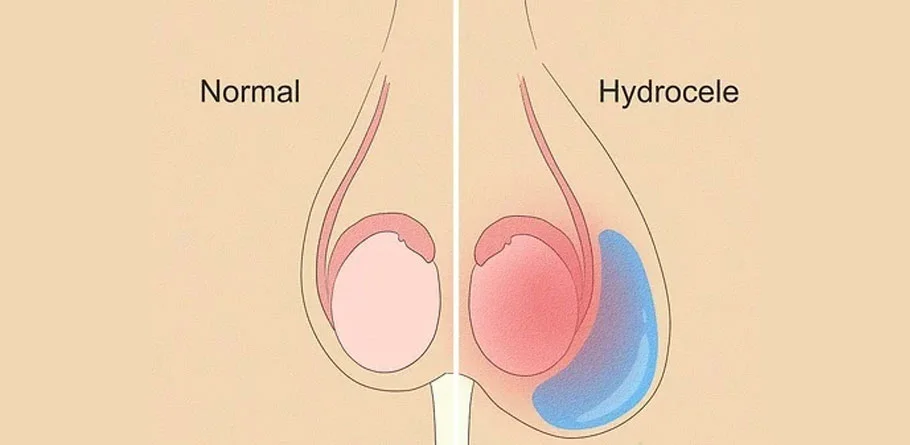
A hydrocele is a common condition characterized by the accumulation of fluid in the scrotum, the sac-like structure that holds the testicles. Normally, a small amount of fluid surrounds the testicles to provide lubrication and allow for movement within the scrotum. However, when this fluid accumulates excessively, it can lead to the formation of a hydrocele.
Hydroceles can occur in males of all ages, from infants to adults, and may present as painless swelling in one or both sides of the scrotum. The swelling may vary in size and can sometimes fluctuate throughout the day, being more pronounced after physical activity or standing for extended periods.
There are two main types of hydroceles:
Communicating Hydrocele:
- In a communicating hydrocele, fluid from the abdomen (peritoneal fluid) flows through a small opening in the abdominal wall into the scrotum. This type of hydrocele is more common in newborns and infants and may resolve spontaneously within the first year of life as the opening closes on its own.
- However, if the communicating hydrocele persists beyond infancy or becomes large enough to cause discomfort or cosmetic concerns, surgical intervention may be necessary to repair the opening and drain the accumulated fluid.
Communicating Hydrocele:
- In a non-communicating hydrocele, fluid accumulates within the layers of tissue surrounding the testicle, typically due to irritation, inflammation, or injury to the scrotum. This type of hydrocele is more common in older children and adults and may develop gradually over time.
- Non-communicating hydroceles are usually painless and may resolve spontaneously, particularly if they are small. However, if the hydrocele persists, causes discomfort, or enlarges significantly, surgical removal of the fluid (hydrocelectomy) may be recommended to alleviate symptoms and prevent complications.
Circumcision

Circumcision
Circumcision is a surgical procedure that involves the removal of the foreskin, the retractable fold of skin that covers the tip of the penis. It is one of the oldest and most commonly performed surgical procedures globally, with cultural, religious, and medical considerations influencing its practice.
Circumcision is performed for various reasons, including:
- Religious or Cultural Beliefs: Circumcision is a common ritual or tradition in many cultures and religions, including Judaism, Islam, and certain African cultures. It is often performed as a rite of passage or as a symbol of identity within these communities.
- Health and Hygiene: Circumcision may offer certain health benefits, such as reduced risk of urinary tract infections (UTIs), sexually transmitted infections (STIs), including HIV, and penile cancer. Removal of the foreskin can make it easier to maintain genital hygiene, as it reduces the accumulation of smegma, a natural lubricant and dead skin cells, beneath the foreskin.
- Medical Indications: In some cases, circumcision may be recommended for medical reasons, such as phimosis (a condition in which the foreskin is too tight and cannot be retracted over the glans), recurrent balanitis (inflammation of the glans and foreskin), or paraphimosis (a condition in which the retracted foreskin cannot be returned to its original position).
Circumcision is performed for various reasons, including:
- Preparation: The patient is prepared for the procedure, which may include administering local anesthesia or general anesthesia, depending on the patient's age and medical condition.
- Surgical Removal: The surgeon carefully removes the foreskin using a scalpel or surgical scissors. The extent of foreskin removal may vary depending on cultural, religious, or medical preferences.
- Hemostasis and Closure: Any bleeding vessels are cauterized or tied off to prevent bleeding, and the remaining edges of the skin are sutured together using dissolvable stitches.
- Postoperative Care: After the procedure, the patient may be given pain medication and instructions for wound care. It is essential to keep the area clean and dry during the healing process to prevent infection.
Piles/ Fissures
Piles/ Fissures
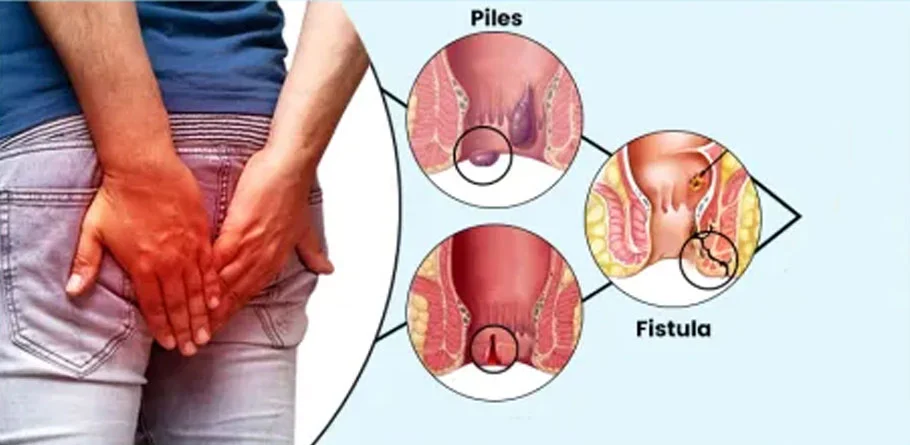
Piles, also known as hemorrhoids, and anal fissures are two common conditions affecting the anal region, each with distinct characteristics and causes. While they both can cause discomfort and pain, they differ in terms of their symptoms, presentation, and treatment approaches.
Piles (Hemorrhoids):
- Piles are swollen and inflamed veins in the rectum and anus that can cause itching, bleeding, and discomfort, particularly during bowel movements. They can occur internally, inside the rectum, or externally, under the skin around the anus.
- Common causes of piles include straining during bowel movements, chronic constipation or diarrhea, obesity, pregnancy, and prolonged sitting or standing.
- Symptoms of piles may include pain, itching, bleeding during bowel movements, swelling or lumps around the anus, and mucus discharge.
- Piles are classified into four grades based on their severity, ranging from grade I (small swellings inside the rectum) to grade IV (large, permanently prolapsed piles).
- Treatment for piles depends on the severity of symptoms and may include lifestyle modifications such as dietary changes, increased fiber intake, and topical treatments to reduce inflammation and relieve symptoms. In more severe cases, procedures such as rubber band ligation, sclerotherapy, infrared coagulation, or surgical removal may be necessary to alleviate symptoms and prevent complications.
Anal Fissures:
- Anal fissures are small tears or cracks in the lining of the anal canal, typically caused by trauma during bowel movements, passing hard stools, or straining. They can result in pain, bleeding, and discomfort, particularly during or after bowel movements.
- Common symptoms of anal fissures include sharp or burning pain during bowel movements, bright red blood on the toilet paper or in the stool, itching or irritation around the anus, and spasms of the anal sphincter muscles.
- Anal fissures are usually diagnosed based on symptoms and physical examination. In some cases, additional tests such as an anoscopy or sigmoidoscopy may be performed to evaluate the extent of the fissure or rule out other conditions.
- Treatment for anal fissures often involves conservative measures such as dietary changes to soften stools, topical treatments to relieve pain and promote healing, and sitz baths to soothe the affected area. In cases where conservative measures fail to provide relief, medical procedures such as botulinum toxin injection, topical nitroglycerin, or surgical repair may be considered.
Abscess Drainage
Abscess Drainage
Abscess drainage is a medical procedure used to remove pus and fluid from an abscess, a localized collection of pus that forms within tissues as a result of infection, inflammation, or trauma. Abscesses can occur in various parts of the body, including the skin, internal organs, and deep tissue spaces, and they can cause pain, swelling, redness, and fever.
The drainage of an abscess is typically performed to alleviate symptoms, promote healing, and prevent complications such as spread of infection, tissue necrosis, or systemic illness. The procedure involves the following steps:
- Preparation: Before the drainage procedure, the patient's medical history is reviewed, and a physical examination is performed to assess the size, location, and severity of the abscess. Imaging tests such as ultrasound or CT scan may be used to visualize the abscess and determine its depth and extent.
- Anesthesia: Local anesthesia is usually administered to numb the area around the abscess and minimize discomfort during the procedure. In some cases, sedation or general anesthesia may be used, particularly if the abscess is large or located in a sensitive area.
- Incision: Once the area is numb, the healthcare provider makes a small incision (cut) over the abscess to create an opening through which the pus can be drained. The incision is carefully made to ensure adequate drainage and minimize damage to surrounding tissues.
- Pus Removal: Using gentle pressure or suction, the pus and fluid within the abscess are drained out through the incision. In some cases, the healthcare provider may insert a drainage catheter or leave the incision open to allow continuous drainage and prevent re-accumulation of fluid.
- Wound Care: After the pus has been drained, the abscess cavity is irrigated with saline solution to clean the area and remove any remaining debris or bacteria. The wound may be packed with sterile gauze or left open to heal from the inside out, depending on the size and depth of the abscess.
- Dressing and Follow-up: Once the drainage procedure is complete, the wound is covered with a sterile dressing to protect it from infection and promote healing. Patients are instructed on how to care for the wound at home, including keeping it clean and dry, changing dressings as needed, and monitoring for signs of infection or recurrence.
Debridement (Bedsores, Diabetic Foot)

Debridement (Bedsores, Diabetic Foot)
Debridement is a medical procedure used to remove dead, damaged, or infected tissue from wounds, ulcers, or other areas of the body to promote healing and prevent infection. It is commonly employed in the management of conditions such as bedsores (pressure ulcers) and diabetic foot ulcers, where tissue necrosis and impaired wound healing can occur.
Bedsores (Pressure Ulcers):
- Bedsores, also known as pressure ulcers or decubitus ulcers, are areas of damaged skin and underlying tissue that develop due to prolonged pressure or friction on the skin, typically over bony prominences such as the heels, hips, or sacrum.
- Debridement is often necessary to remove necrotic (dead) tissue, slough (yellow or white fibrinous material), and eschar (dry, black necrotic tissue) from the ulcerated area, as these materials can impede wound healing and increase the risk of infection.
- Debridement techniques used for bedsores may include sharp debridement (using surgical instruments such as scalpels or scissors to remove dead tissue), mechanical debridement (using dressings, irrigation, or wet-to-dry dressings to mechanically remove necrotic tissue), enzymatic debridement (applying topical enzymes to break down necrotic tissue), or autolytic debridement (using the body's own enzymes and moisture to dissolve dead tissue).
Diabetic Foot Ulcers:
- Diabetic foot ulcers are chronic wounds that develop on the feet of individuals with diabetes, often as a result of neuropathy (nerve damage), poor circulation, and impaired wound healing. These ulcers can lead to serious complications such as infection and lower limb amputation if not properly managed.
- Debridement plays a crucial role in the treatment of diabetic foot ulcers by removing non-viable tissue, reducing bacterial load, and promoting granulation tissue formation. It helps create a clean wound bed that is conducive to healing and reduces the risk of infection.
- Similar debridement techniques used for bedsores may be employed for diabetic foot ulcers, including sharp, mechanical, enzymatic, or autolytic debridement, depending on the characteristics of the wound and the patient's overall health status.

Minimal Invasive Surgery
Minimally invasive surgery (MIS), also known as laparoscopic or keyhole surgery, refers to surgical techniques that involve performing procedures through small incisions instead of larger, traditional incisions used in open surgery. The primary goal of minimally invasive surgery is to minimize trauma to the body's tissues, reduce postoperative pain, shorten recovery time, and improve overall patient outcomes.
In minimally invasive procedures, surgeons utilize specialized instruments, cameras, and advanced technology to access the surgical site through small incisions, typically ranging from a few millimeters to a few centimeters in size. A tiny camera called a laparoscope is inserted through one of the incisions, providing a magnified, high-definition view of the surgical area on a monitor. This allows surgeons to visualize internal structures with precision and perform the necessary manipulations using long, slender instruments inserted through other small incisions.
Minimally invasive surgery can be applied to a wide range of surgical procedures across various medical specialties, including general surgery, gynecology, urology, orthopedics, and thoracic surgery. Some common minimally invasive procedures include laparoscopic cholecystectomy (gallbladder removal), laparoscopic appendectomy (appendix removal), laparoscopic hernia repair, laparoscopic hysterectomy (removal of the uterus), and minimally invasive prostate surgery.
Benefits of minimally invasive surgery may include:
- Reduced trauma to surrounding tissues and organs.
- Smaller incisions, leading to less scarring.
- Decreased postoperative pain and discomfort.
- Shorter hospital stays and faster recovery times.
- Lower risk of complications such as infection and bleeding.
- Improved cosmetic outcomes.
Gastrointestinal Surgery
Gastrointestinal (GI) surgery is a specialized field of surgery that focuses on the diagnosis and treatment of disorders affecting the digestive system, including the esophagus, stomach, small intestine, large intestine (colon), liver, pancreas, gallbladder, and rectum. GI surgeons are trained to perform a wide range of procedures to address conditions such as cancer, gastrointestinal reflux disease (GERD), inflammatory bowel disease (such as Crohn's disease and ulcerative colitis), diverticulitis, gallstones, and hernias affecting the abdominal region.
Here are some common types of gastrointestinal surgeries:
- Esophageal Surgery: This involves procedures to treat conditions affecting the esophagus, such as esophageal cancer, gastroesophageal reflux disease (GERD), and achalasia. Surgical options may include esophagectomy (removal of part or all of the esophagus) and fundoplication (to treat severe GERD).
- Stomach Surgery: Procedures related to the stomach include gastrectomy (partial or total removal of the stomach), often performed to treat stomach cancer, and gastric bypass surgery for severe obesity.
- Intestinal Surgery: This encompasses surgeries involving the small intestine and colon. Common procedures include bowel resections for conditions like Crohn's disease, ulcerative colitis, and colorectal cancer, as well as surgeries to treat bowel obstructions, diverticulitis, and hemorrhoids.
- Liver Surgery: Liver surgery may involve resection of liver tumors (hepatectomy), liver transplant for end-stage liver disease, and surgical procedures to address liver abscesses or cysts.
- Pancreatic Surgery: Pancreatic surgeries are performed for conditions such as pancreatic cancer, chronic pancreatitis, and pancreatic cysts. Procedures may include pancreaticoduodenectomy (Whipple procedure), distal pancreatectomy, or total pancreatectomy.
- Gallbladder Surgery: Cholecystectomy, the removal of the gallbladder, is one of the most common gastrointestinal surgeries and is typically performed to treat gallstones or gallbladder inflammation (cholecystitis). It can be done through traditional open surgery or laparoscopically.
- Anorectal Surgery: This involves procedures to treat conditions affecting the anus and rectum, such as hemorrhoids, anal fissures, fistulas, and rectal prolapse.
HPB Surgery
HPB surgery stands for Hepatopancreatobiliary surgery, which is a highly specialized field of surgery that focuses on the diagnosis and treatment of diseases affecting the liver, pancreas, and bile ducts. HPB surgeons are skilled in performing complex surgical procedures to treat a variety of conditions, including benign and malignant tumors, cysts, infections, and anatomical abnormalities within these organs and their associated structures.
- Liver Surgery: HPB surgeons perform liver resections (hepatectomies) to remove portions of the liver affected by tumors (both primary and metastatic), cysts, or other diseases. They may also perform liver transplantations for end-stage liver disease caused by conditions such as cirrhosis, hepatitis, or liver cancer.
- Pancreatic Surgery: HPB surgeons are trained in performing surgeries on the pancreas to treat conditions such as pancreatic cancer, pancreatitis (both acute and chronic), pancreatic cysts, and pancreatic neuroendocrine tumors. Procedures may include pancreaticoduodenectomy (Whipple procedure), distal pancreatectomy, or total pancreatectomy, depending on the specific diagnosis and extent of the disease.
- Biliary Surgery: This involves surgical procedures to address diseases affecting the bile ducts and gallbladder. HPB surgeons may perform procedures such as bile duct resections, hepaticojejunostomy (surgical reconstruction of the bile ducts), or cholecystectomy (removal of the gallbladder) for conditions like bile duct strictures, choledochal cysts, or gallstones.
- Minimally Invasive Techniques: Like in other surgical specialties, HPB surgeons are increasingly utilizing minimally invasive techniques, such as laparoscopy and robotic-assisted surgery, to perform complex HPB procedures. These techniques offer benefits such as smaller incisions, reduced postoperative pain, shorter hospital stays, and faster recovery times compared to traditional open surgery.